

Shane Horan is an author (The Confidence Interval) and engineer in the pharmaceutical industry. Follow him on Twitter @shane1horan.
So imagine a bunch of aliens come to earth and decide to run a hospital emergency room (I promise this is going somewhere). They don't know anything about human physiology, but they've got a good grounding in empirical principles, and a can-do attitude.
The part of town where they set up has a big knife crime problem. Knife crime doesn't exist on their planet, so they don't understand what's happening when people stagger in the door with a dark red liquid soaking their clothes. These patients often die soon after! In fact, the ones with the most red liquid on their clothes tend to die the fastest. They surmise that the dying is related to the red-liquid-soaked clothes, and they come up with a plan.
The best alien scientists examine the red liquid and determine its structure. They try different methods to remove the blood. Finally they develop an enzyme-based treatment, which when applied to the outside of the human dissolves the blood instantly.
The clinical trials were disappointing.
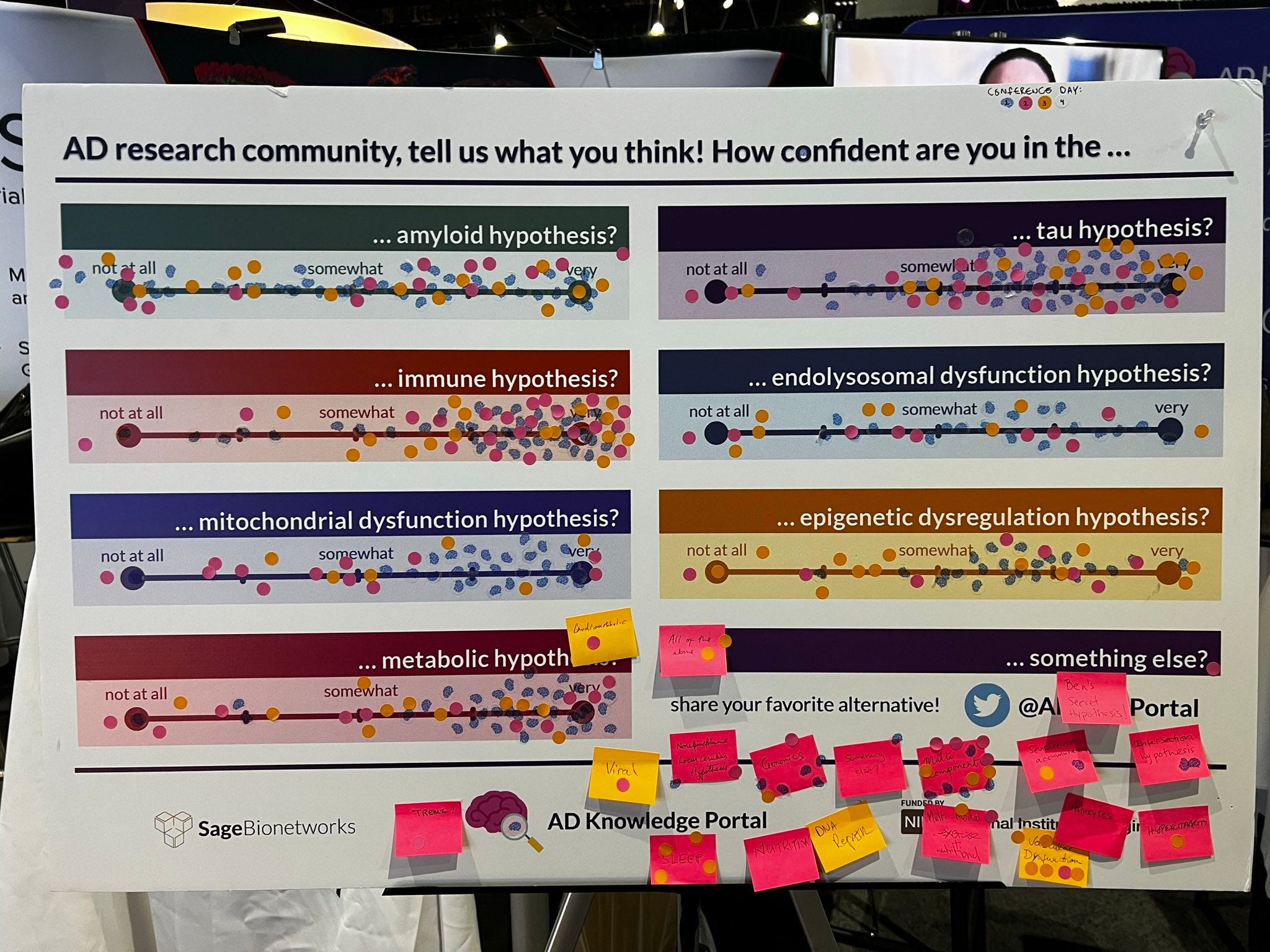
The Alzheimer's Association International Conference is the leading scientific conference for Alzheimer's Disease (AD) researchers. The poster above is from the 2022 conference in San Diego. It's a kind of visual poll, where participants were asked to rate their confidence in the various hypotheses for the cause of Alzheimer's. You place a coloured dot on a line between "very" and "not at all" (each day used a different colour dot).
First impression - there are dots everywhere! Every hypothesis has at least a few dots around "very confident" and a few around "not at all confident". In addition to the 7 main hypotheses, there are more write-in candidates on the post-its - Viral, Senescence Accumulation, Sleep, Vascular Dysfunction and All Of The Above each get a few votes.
Isn't this surprising? AD was first described more than a hundred years ago. It affects millions of people worldwide and is a leading cause of death in developing countries. Shouldn't we know what causes it, rather than having a dozen viable hypotheses?
Have a look at the top left - the amyloid hypothesis. It has votes all over the confidence range. Some at the upper end, but some off the scale at the bottom end! So what is the amyloid hypothesis and why is it so divisive?
If you study the brains of people who died from AD, you find plaques made of a protein which has been excreted from neurons and misfolded into irregular clumps.
(How a protein folds is a critical part of how it works. The chain of amino acids produced by a ribosome based on the genetic instructions it receives, is essentially a 1-dimensional string. It is only by folding that string into 2-dimensional ribbons & sheets, and then further into 3-dimensional structures, that the protein becomes functional).
The protein is called amyloid beta. It seems to be present in 100% of AD cases, and as the disease progresses, the number of plaques increases. The amyloid hypothesis is that the accumulation of amyloid is part of the causal chain that ends in cognitive decline and death:

The amyloid plaques are thought to accumulate as we age, forming more or less quickly based on genetic susceptibility and other factors.
Amyloid is definitely part of the puzzle. But is it like the bloodied clothes in the alien ER: an obvious external sign of disease, but not causal?
Typical AD is maddeningly unpredictable. It seems to effect very many people eventually, but it strikes some people much earlier than others, for no obvious reasons. This is why the typical form is known as sporadic AD. But if we look at atypical cases, there are clues that suggest amyloid might be causal. People with Down syndrome have a third copy of APP (the gene that codes for the amyloid protein) as the gene is on their trisomic chromosome 21. And it turns out they also get amyloid accumulations and Alzheimer's earlier than others.
The non-sporadic minority of AD cases are known as familial. These are cases that can be linked clearly to a faulty version of a single gene. Some inherited mutations of the APP gene cause familial AD. The so-called Swedish mutation causes increased production of amyloid. So that fits nicely into the causal chain above:

But the Swedish mutation only accounts for a minority of familial AD, which itself is only a minority of all AD cases. Most familial cases are caused by different mutations in APP, or different genes entirely, whose relationship to amyloid is less straightforward.
Some mutations are believed to affect the folding and slicing of the amino acid chain which produces the final amyloid protein. So instead of producing the correct form of amyloid, so-called toxic oligomers are formed. A variation of the amyloid hypothesis proposes that in the typical sporadic form of AD too, it's not the amount of amyloid produced that causes the amyloid plaques, it's the type of amyloid.
One of the best-studied oligomers is (or was) Aβ*56 ("amyloid beta star fifty-six"). Sylvain Lesné at the University of Minnesota claimed in 2006 to have isolated this oligomer, and proved that it directly caused memory impairment when injected into rats. Lesné produced a string of exciting results, which caused some in the field to believe they were finally closing in on the cause of Alzheimer's. Until it all came crashing down.
Other scientists had trouble replicating his results. In fact, they had trouble even isolating Aβ*56, and some even doubted it was possible. Other groups failed to find Aβ*56 in any human tissues. And then neuroscientist Matthew Schrag made the final swing of the axe that toppled Aβ*56: he found dozens of apparently doctored images in Lesné's papers. Images which were meant to represent independent runs of western blots (a protein analysis technique) appear to have sections that have simply been copied and pasted. The image manipulations appear across 10 papers about Aβ*56 spanning more than a decade of highly-touted research, and another 10 articles by Lesné. (See this excellent long read in Science by Charles Piller for the complete story). The reaction from the journals and institutions involved has been surprisingly quiet. No papers have been retracted. Some have had images of concern replaced, but some of the replaced images also showed signs of tampering! And Lesné still has a job (but presumably little credibility).
It's not hard to see why confidence in the amyloid hypothesis is low, when some of the most promising research in the area turns out to be built on something very close to outright scientific fraud. And there are more problems in the area, alluded to in the Science article and described in detail in this STAT News piece by Sharon Begley. Over and over, researchers who tried to investigate alternatives to the amyloid hypothesis report trouble getting funded or published. The Science piece mentions an "amyloid mafia", the STAT piece a "cabal". The wording is emotive, and as Begley points out the "cabal" are not sinister agents trying to suppress the truth. They are the reviewers of papers, the editors of journals and the principal investigators at AD labs. They are the true believers in amyloid, who want to accelerate research past the hypothesis-generation stage and into developing real treatments, based on the leading hypothesis (as they see it). But they have collectively, inadvertently, suppressed research into alternative hypotheses.
And they have been successful. Almost every drug which has made it to clinical trials has targeted amyloid. And almost every drug has failed. Two have made it past FDA approval - aducanumab and lecanemab. They have shown an ability to reduce amyloid plaques. But they have shown very, very modest ability to slow the cognitive decline of Alzheimer's. Which is what we actually care about!
I should mention that studies on another amyloid targeting drug, donanemab, have claimed a 35% reduction in the rate of cognitive decline. This would certainly be a boost for the amyloid hypothesis, and for AD sufferers, if it pans out. As Begley notes, targeting amyloid may be necessary for curing AD, but it seems unlikely to be sufficient. Surely if we really want to cure AD, rather than just delay it, we need to find the root cause - the things that appear before "More Amyloid Produced" in the causal chain. And the desire to know more is clearly there among researchers - look at all the interest in other hypotheses in the conference poll. They need to be supported to do exploratory research, not based on wobbly prior research but on an open-minded and realistic assessment of what we truly know. If we simply rush to treat patients for the most obvious external sign of their disease, without a complete understanding, we are just cleaning the blood from stab victims' clothes.
It would seem that treating the Amyloid Plaque problem is just treating a symptom and not a cause of AD. Are we making the researchers happier by acknowledging this approach? It does not help the patient and is not preventative. Once again medical research is treating a visible sign of the disease (an observable symptom) and not the disease itself. Has anyone looked into why "Donanemab" works differently?
... aducanumab, lecanemab, donanemab...
O, then, I see Queen Mab hath been with you.
She is the fairies' midwife, and she comes
In shape no bigger than an agate stone...
And in this state she gallops night by night
Through lovers' brains, and then they dream of love;
O'er scientists' laptops, that dream on citations straight,
Sometime she driveth o'er a pharma boss’s neck,
And then dreams he of clinical trials, of FDA approval,
Of healths five-fathom deep; and then anon
Drums in his ear, at which he starts and wakes,
And being thus frighted swears a prayer or two
And sleeps again. This is that very Mab
That plats the amyloids in the night...